Glaucoma is not a contagious disease; you can’t get it from being near someone who has it. And there are no specific behaviors or environmental influences that are known to be causes of glaucoma. Even so, it affects close to 2% of the U.S. population over age 40, and anyone can develop the condition.
There are several different types of glaucoma, but they can be divided into two broad categories. The first category is primary glaucomas. They are called primary because they develop on their own, without any known cause. Most cases fall into this category.
The other category is secondary glaucomas. They are called secondary because they develop as a result of something else that came first. Causes of secondary glaucoma range from congenital birth defects to eye infections.
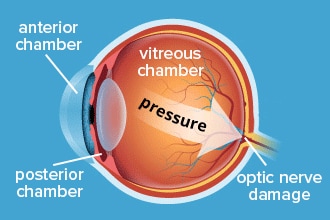
Having high internal eye pressure (called ocular hypertension) is one major risk factor in both categories. In the majority of cases, it is clear that high eye pressure ultimately led to cell death in the optic nerve.
However, for many people, moderately high IOP never affects these cells. Others develop glaucoma even though their IOP has always been within a normal range. And in some patients, the nerve cell damage keeps progressing after treatment lowers their IOP.
Even with these differences, elevated IOP is still the most important risk factor for glaucoma. The higher the IOP, the higher the risk — and very small increases in IOP can raise a person’s risk by up to 10%.
Researchers have not yet been able to solve why eye pressure affects the optic nerve differently in different people. Some of the most long-standing theories are that eye size, eye wall thickness and the optic nerve’s blood supply may be involved. Another is that some optic nerves may simply be more sensitive.
Relatively newer research over the last 20 years points to other possible causes of glaucoma at the molecular level.
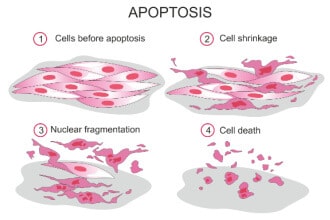
When retinal ganglion cells die, it often happens through a process called apoptosis. This is a natural process that causes aging, damaged or abnormal cells to self-destruct. In glaucoma, stress on the optic nerve cells from IOP triggers this process.
There is evidence that differing amounts of stress on these cells can cause molecular changes in their extracellular matrix (ECM).
The ECM surrounds cells and is made up of proteins that support cell structure and regulate cell behavior.
Researchers theorize that various changes in the ECM could be responsible for if and when apoptosis is triggered.
There is also evidence that one of the causes of glaucoma may be an autoimmune dysfunction.
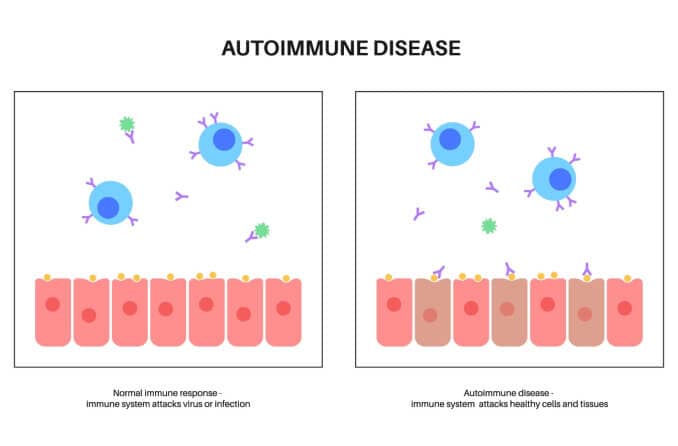
Normal immune response v. autoimmune response
Researchers have found that retinal ganglion cells produce heat shock proteins (HSPs)in response to stress.
HSPs typically act as protection for cells. But in glaucoma, it appears that these HSPs are triggering an autoimmune T-cell response.
The flood of T-cells may be what ultimately leads to RGC death.
Though there are no definitive answers about the causes of glaucoma, lowering IOP is the main target in treatments. Most, if not all, forms of the disease are related to IOP in some way.
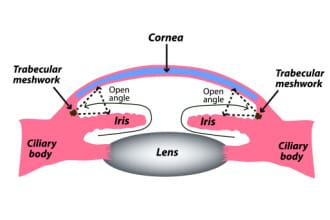
Primary open-angle glaucoma (POAG)
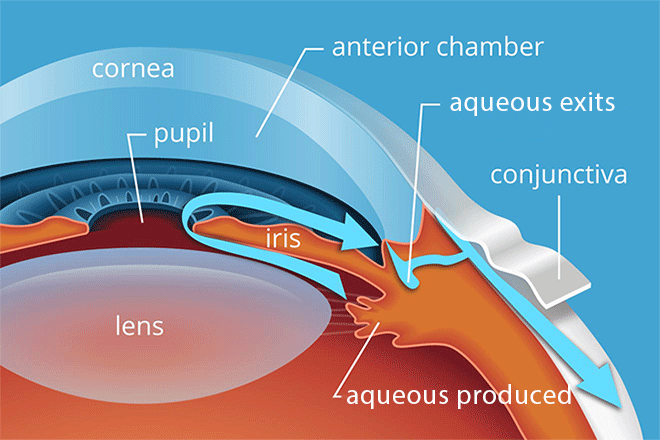
This form usually develops due to structural changes in the trabecular meshwork (TM)or, less often, in Schlemm’s canal. It’s called open-angle because nothing is blocking or restricting the eye’s drainage angle.
Instead, the tissues of the TM become stiff, or the number of its sponge-like pores decreases. These changes make it difficult for aqueous humor to pass through, and then IOP goes up.
Primary open-angle glaucoma (POAG) is the most prevalent type in the U.S., accounting for up to 95% of all glaucoma. It is the second-highest cause of blindness among Black Americans after cataracts. For white Americans, it is the third-highest cause of blindness after AMD and cataracts.
If POAG is detected early, it’s possible for many patients to avoid significant vision loss. But POAG rarely has symptoms, and it progresses very slowly. An estimated 50% of people never realize they have it until they experience significant loss of vision. The only way to catch it early is to have yearly comprehensive eye exams.
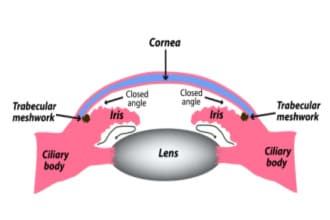
Primary angle-closure glaucoma (PACG)
This form is also called narrow-angle glaucoma. It develops when the outer edge of the iris shifts and blocks the drainage angle. Though it gets its name from this blockage, it usually results from a problem earlier in the aqueous outflow path.
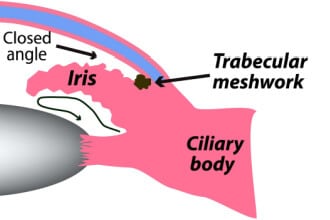
The underlying cause of narrow angles is usually pressure behind the iris that causes the iris to bow forward. When the iris is bowed, its outer edge is pushed forward and toward the angle. And its inner edge, which forms the pupil, is pulled backward toward the lens.
With the pupil’s edge closer to the lens, less fluid can pass through its opening. This is called pupillary block. Pupillary block causes fluid to accumulate behind the iris and leads to even more bowing and angle narrowing.
In most cases, eyes that develop pupillary block and PACG already have less space between the lens and iris.
It may be due to anatomical factors, such as having naturally large lenses or thicker irises. Having smaller-than-average eyes can have the same effect if the lens and iris are too crowded in the small space. Age plays a role as well — the lens of the eye continues to grow as we get older.
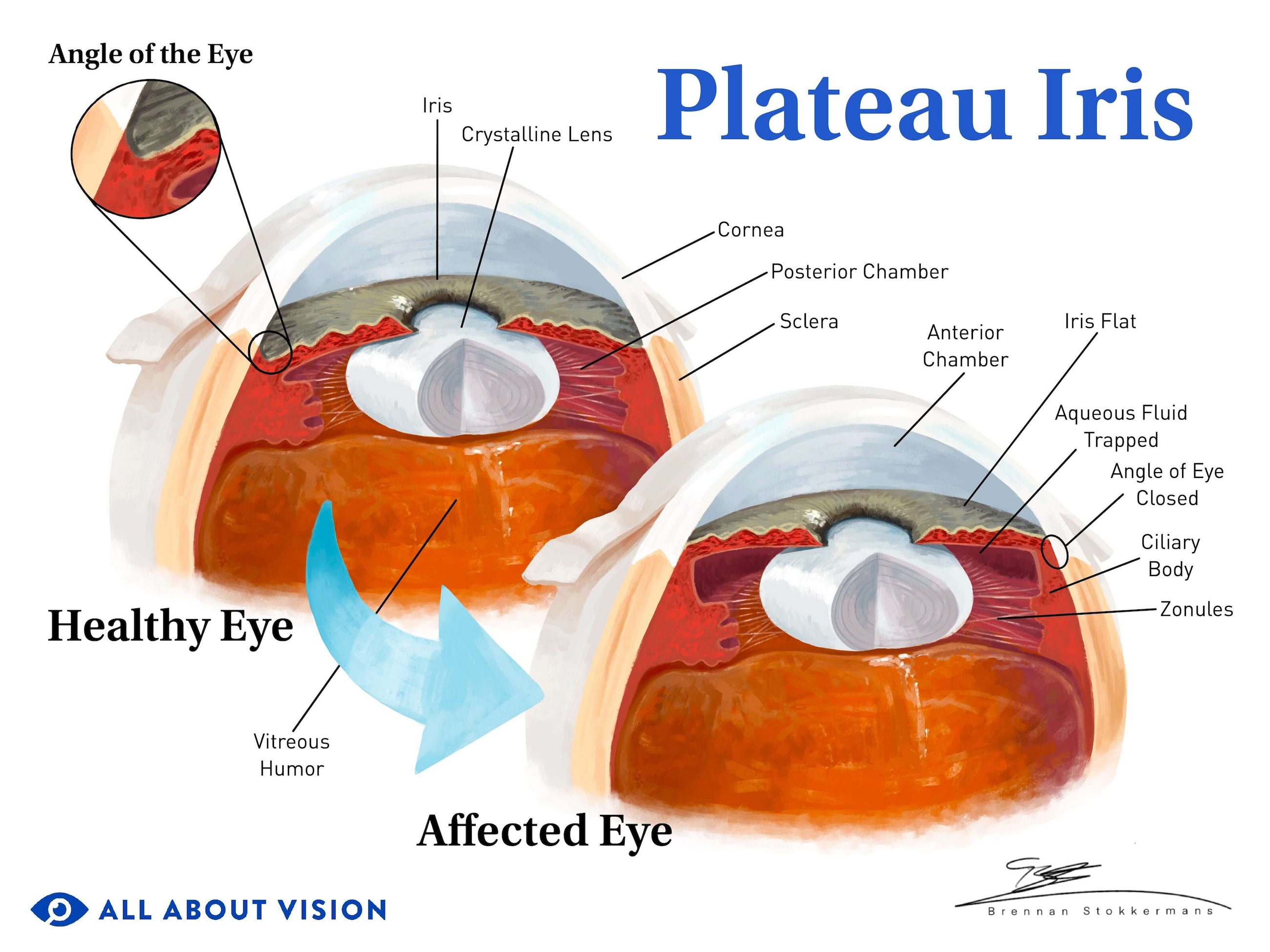
PACG can also occur without pupillary block. Some eyes have naturally narrow angles due to an anatomical trait known as plateau iris.
In these eyes, there is plenty of space between the lens and iris. Instead, the size or forward placement of the iris and/or ciliary body crowd the drainage angle.
The most common treatment for angle-closure glaucoma — a peripheral iridotomy — does not work for plateau iris. It is difficult to diagnose and requires an eye doctor who is experienced in gonioscopy. Misdiagnosis can lead to rapid vision loss.
ACG is usually chronic, meaning it progresses slowly, but it can also be acute. The chronic form is the second-most common after POAG and rarely has symptoms.
The acute (sudden)form is much less common, but it does have symptoms and is very serious. An acute attack can cause intense eye pain, blurry vision, and nausea or vomiting. Untreated acute angle-closure glaucoma causes blindness within hours or days. It is a medical emergency that needs to be treated immediately.
Primary congenital glaucoma (PCG)
This form occurs due to problems during the development of the eye’s drainage system. Babies with primary congenital glaucoma (PCG)often have obvious signs of the condition at birth, such as abnormally large eyes or clouded corneas.
This is because the built-up fluid and pressure has stretched and enlarged the eyes. But some babies born with PCG have later onsets of these signs that range from a few weeks up to around two years.
PCG is one of two types of primary childhood glaucoma. The other is juvenile open-angle glaucoma (JOAG). It is also congenital, but its onset tends to be later in early childhood. Children diagnosed with JOAG are less likely to have enlarged eyes due to this later onset.
Low-tension or normal-tension glaucoma (NTG)
When optic nerve damage develops in eyes that have open angles and typical IOP, it is called normal-tension glaucoma. It is often categorized as a type of POAG.
However, because of its unknown relationship with IOP, some experts disagree that it is truly POAG. They believe it may be a totally separate condition. Either way, normal-tension glaucoma is extremely common.
Approximately 30% to 60% of people with POAG in white and Black populations have normal IOP. It’s even more common among people with POAG in Latino populations (approximately 80%) and Asian populations (47% to 92%).
Some people may develop NTG because their optic nerves have poor blood flow or are more structurally vulnerable to pressure. Another theory is that their eyes are less able to withstand normal pressure due to size, shape, wall thickness or corneal thickness.
It may also be due to an autoimmune issue or to higher sensitivity to typical, daily IOP fluctuations.
Secondary glaucoma
The optic nerve damage that occurs with a secondary glaucoma is the same as in a primary form. The difference between the two is that secondary glaucoma has causes that are distinct and identifiable.
This category is by far the more diverse of the two. Secondary glaucoma can be caused by many things, including underlying health conditions, eye disease and eye injuries. It can also be caused by medication side effects or eye surgery. It can be open-angle or angle-closure, and its different causes can lead to multiple types of glaucoma.
However, even though there are so many types, they only make up about 10% of all diagnosed glaucoma. Some of the more common types include:
The frequency of each type varies across different populations and parts of the world. But the neovascular, exfoliative, pigmentary and steroid-induced forms tend to be among the most common in general.
Neovascular glaucoma (NVG)– NVG is often a result of diabetic retinopathy or other causes of poor blood circulation of the eye. It develops when reduced blood flow to the retina triggers an overgrowth of abnormal blood vessels on the iris that eventually clogs the angle.
Exfoliative & pigmentary glaucoma – These are separate but similar forms caused by exfoliation syndrome (ES)and pigment dispersion syndrome (PDS). Accumulation of abnormal cellular dandruff (with ES) or flakes of iris pigment (with PDS) in the angle lead to high IOP and glaucoma.
Steroid-induced glaucoma – This type develops when steroid use (prescribed and OTC) causes both structural changes and increased debris deposits in the TM. Drainage resistance in the TM increases IOP and leads to glaucoma.
LEARN MORE about the types and causes of secondary glaucoma
 and optic nerve damage")






")

